EHR Optimization
Arch CollaborativeJoin hundreds of healthcare organizations working together to revolutionize healthcare quality by improving the EHR experience
The Arch Collaborative is a group of healthcare organizations committed to improving the EHR experience.
Maximize Your EHR Experience
KLAS works with each member to improve their EHR experience by uncovering opportunities for change through standardized surveys and benchmarking. KLAS meets with members regularly, and the whole Collaborative meets annually to facilitate learning from other healthcare organizations.
Satisfaction ratings for the Acute Care EMR market segment have been lower than the software average for over five years.✝ The Arch Collaborative is working to change this.
✝ Best in KLAS Rankings, 2014-2023
EHR SATISFACTION RESEARCH
Where It All Started
While sifting through our initial Collaborative data, we noticed a pattern that caused us to ask:
How can two organizations using the same EHR report such disparate satisfaction with the user experience?
Percent of Surveyed Clinicians Who Are Satisfied with Their EHR
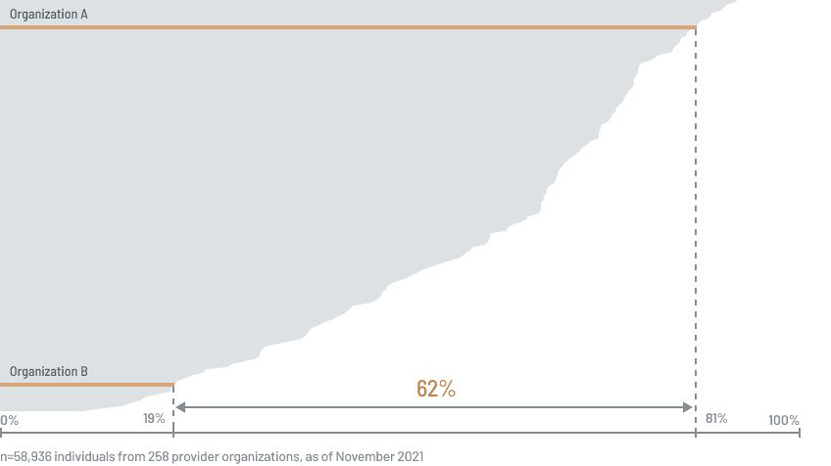
Why is there a 62 percentage points difference between different organizations using the same EHR?
Conclusion
“The truth? All EHRs see a wide spread in user experience from organization to organization. Benchmarking your organization against similiar organizations allows you to find out if you have truly maximized your investment.
This insight led us to dig deeper into what factors are most likely to create satisfied EHR users.
Over and over, the data revealed that satisfied users:
- Are able to personalize their EHR experience
- Share ownership for EHR governance
- Are expert users of their EHR solution

 "Without data, you're just another person with an opinion."
"Without data, you're just another person with an opinion."
— W. Edwards Deming
Benefits of the Arch Collaborative
For Healthcare Organizations
Become a member of the Arch Collaborative to:
- Benchmark EHR satisfaction against similar organizations
- Connect with and learn from other healthcare organizations
- Improve clinician satisfaction with your EHR
- Fine-tune your clinician education
- Alleviate technology-related burnout
- Deliver better care
98% of organizations see an improvement in EHR satisfaction when remeasured. †

† The Science of Improving the EHR Experience 2021, July 2021
Photo by Christina @wocintechchat.com on Unsplash
Photo by Christina @wocintechchat.com on Unsplash
success stories
From the Members Themselves
Real stories from the front-lines. See how the Arch Collaborative made an impact with these healthcare organizations.
University of Kansas Health System
Greg Ator
Chief Medical Informatics Officer and Senior Medical Director
|
“KLAS has reinvigorated my team! Having the voice of the customers—our clinicians—in a benchmark paradigm is imperative to understanding where we, as an organization, are in the journey to provide a superlative clinical computing experience for our users. Otherwise we are in danger of making decisions based on anecdotal or squeaky-wheel feedback. We look forward to maturing this concept to influence all that we do for the clinician experience.” |
Asante
Lee Milligan
Vice-President/Chief Medical Information Officer
|
“The KLAS Arch Collaborative has helped me focus on the often overlooked yet critically impactful influence of EHR usability. Their method of benchmarked analyses combined with linking organizations to learn from one another has set a new standard for both EHR design and training collaboration in this space. It’s powerful to work together to get this right.” |
Penn Medicine
Michael Restuccia
Senior Vice President and Chief Information Officer
|
“The KLAS Arch Collaborative survey and program provide unbiased insights regarding clinician utilization and adoption of the electronic medical record along with practical recommendations to enhance these metrics across your healthcare enterprise. If you don’t know where you stand, it’s difficult to improve and become world-class.” |
WellStar Medical Group
Rob Schreiner
President
|
“The Collaborative allows us to benefit from the wisdom, hard work, and objective results of other health systems. As a result, we get better faster.” |
Sydney Local Health District
Aaron Jones
Chief Nursing and Midwifery Information Officer
|
“The Arch Collaborative is important for our team because we understand where our current eMR install is at and what we can do to improve. We have found great value in collaborating with other organisations and learning from their best practices. We encourage other organisations to join this effort.” |
Advocate Aurora Health
Robert Whitcomb
Chief Medical Information Officer, Perioperative Medical Informatics
|
“We found that the Arch Collaborative both affirmed our work and gave us meaningful feedback on how we could improve. The power of the data helped guide our efforts.” |
The Ohio State University Wexner Medical Center
Milisa Rizer
Chief Clinical Information Officer
|
“The Arch Collaborative has helped us assess the needs of our users and reach out to very specific areas to address those needs. The collaborative opportunity that the Arch Collaborative brings to the community of information technology in healthcare is changing how we think about interacting with electronic medical records now and in the future.” |
UC Davis Health
Scott MacDonald
EHR Medical Director
|
“The Arch Collaborative has given us a different approach to consider our own internal data that is very useful. Sharing our data with their experts gave us a critical sounding board to refine and contextualize our local work.”healthcare is changing how we think about interacting with electronic medical records now and in the future.” |
Compass Medical
Dhrumil Shah
Chief Medical Information Officer
|
“Being part of the Arch Collaborative has created new opportunities for our organizational success. We have immersed ourselves in learning experiences that probably won’t feel comfortable at first given the challenges we all face in the healthcare industry, but the power of data-driven insights is giving us opportunities and making us nimble with that new knowledge.” healthcare is changing how we think about interacting with electronic medical records now and in the future.” |
how to participate
Become a Member
Real leadership requires data. Put the insights of over 200,000 clinician respondents at 250+ healthcare organizations to use.

Express your interest.
Discuss membership options.

 See Sample Benchmark Survey
See Sample Benchmark Survey

250+
Healthcare organizations
and counting
Healthcare organizations
and counting
14+
Healthcare IT companies
and counting
Healthcare IT companies
and counting
Become a Collaborative member. Start your EHR improvement journey today.
Benefits of the arch collaborative
For Healthcare IT Companies (Vendors)
Use Arch Collaborative findings to give your solutions the edge they need to excel.
Get Crucial Information
- Key pain points using the EHR
- Best practices that drive high user satisfaction
- Tips for improving clinician efficiency
Proactively Optimize
- Fix problems before they become detrimental
- Help customers deliver better healthcare
Express Interest
- Reach out to our vendor specialist if you have any questions or would like to participate.
Vendor Participation
By participating in the Collaborative, healthcare IT companies can dramatically reduce the time it takes to implement changes based on end-user feedback.
Recent Research